 Radiologists agree on the importance of breast cancer screening and are taking steps to improve access and empower women to make informed decisions. Click here to see steps you can take in your community and practice.
Radiologists agree on the importance of breast cancer screening and are taking steps to improve access and empower women to make informed decisions. Click here to see steps you can take in your community and practice.
Each year, Arizona resident Michelle Ochenkoski dreads scheduling her annual mammogram. “It fills me with fear and anticipation, because every year they see something questionable on my mammogram,” Ochenkoski says. “It creates a lot of stress and anxiety.”
Ochenkoski is among the 50% of all women who have dense breast tissue, which can mask tumors on a mammogram and can also increase a woman’s risk of developing breast cancer. Recognizing these factors, Arizona legislators approved a
mandate in 2014 that requires healthcare providers to notify patients, like Ochenkoski, whose mammography results indicate that they have dense breast tissue.
The only problem was that Ochenkoski, like many women, didn’t understand what the notification meant, so she just tucked it away in her medical file with everything else.
But after Ochenkoski’s mammogram this year, her primary care physician (PCP) asked if she’d like to visit the new dense breast consultation clinic at the Mayo Clinic in Arizona to speak to a radiologist about the implications of dense breast tissue and explore additional screening options. Ochenkoski eagerly agreed.
“It was such an eye-opener to really understand how dense breast tissue appeared on my mammogram, and what else the radiologist could see with additional imaging,” she says. “The consultation made such a big impact on me that I decided to get additional imaging so I could finally have an answer to my questions about breast health.”
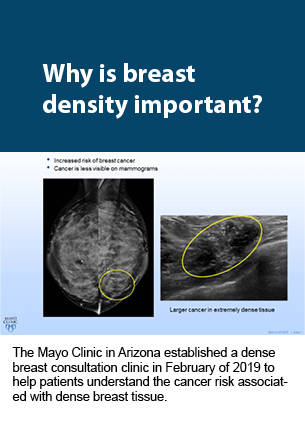
Since Mayo opened its dense breast consultation clinic in February of 2019, more than 140 patients have scheduled appointments to speak directly with a radiologist about their breast density. Leveraging the radiologists’ expertise, the program has helped women better understand the correlation between dense breast tissue and increased cancer risk, empowering them to make more informed breast imaging decisions.
Identifying the Gap
After Arizona and several other states mandated that healthcare providers send notifications to patients who have dense breasts, the president signed a similar directive into federal law in February of 2019. The notifications encourage patients with dense breast tissue to discuss additional screening options with their physicians — typically PCPs, OB/GYNs, and internists — who don’t always have the imaging expertise needed to explain the tests.
“A lot of confused women come to us asking, ‘What does this mean? Do I need to do additional imaging?’” says Jewel Kling, MD, MPH, NCMP, associate professor of medicine and associate chair for research in women’s health internal medicine at the Mayo Clinic in Arizona. “It creates challenges in a primary care setting, because we have limited time to spend with patients, and even a five-minute conversation about breast density becomes a battle of priorities.”
As a result, referring physicians like Kling frequently called Victor J. Pizzitola, MD, MPH, division chair of breast imaging at the Mayo Clinic in Arizona to ask him how to respond to patients’ questions about supplemental screening. He didn’t have an immediate solution for streamlining the process — but a few years later, when fourth-year resident, Kristin A. Robinson, MD, asked how she could get more involved in patient care during her breast imaging fellowship, it suddenly clicked. As Pizzitola and Robinson brainstormed ideas, they realized that a dense breast consultation clinic could be the perfect opportunity for radiologists to add value.

“We realized there was a gap because the notification told patients to talk with their doctors, but their PCPs and OB/GYNs may not have the updated knowledge on supplemental screening exams — or even the time to have a breast density conversation,” Robinson says. “We wanted to address it in a way that was helpful to both the referring provider and the patient by establishing a consultation clinic to fill that gap. Breast imagers were already having these types of conversations with patients, so this created a more formal environment to share our expertise.”
Making a Case for Consultation
Early in the planning process, Pizzitola identified the top five mammography referrers at the Mayo Clinic in Arizona and asked them what they thought of the idea. Their immediate reaction was relief. “Opening that dialogue with our referring providers was critical because it helped us understand how ill-equipped they were to discuss breast density with patients,” Pizzitola says. “Creating the consultation clinic took the onus off referring providers and allowed the radiologists the opportunity to share their knowledge with patients directly.”
When Pizzitola introduced the idea to other radiology leaders at the Mayo Clinic in Arizona around June of 2018, they agreed that it would advance the practice and improve patient care. But as he began meeting with hospital administrators, he hit some logistical roadblocks. “The immediate answer we got from the administrators in finance and billing was, ‘No. Radiologists can’t see patients, because they can’t chart or bill for this,’” Pizzitola says.
To convince administrators of the idea’s potential, Pizzitola diagramed the clinic’s workflow, from ordering to billing. He reached out to a breast imaging colleague at another Mayo Clinic location who had experience with billable evaluation and management consultations. This colleague explained how radiologists could perform, chart, and bill for consultations, and how referring physicians could order them through the electronic medical record (EMR). Pizzitola and Robinson used this information to create a business plan with a financial impact analysis.
“In order to make this viable and long-lasting after my fellowship, we had to show our institution that if we’re taking a radiologist’s valuable time away from the reading room, at least we can be reimbursed for the additional service we’re providing,” Robinson says. “Although it is revenue-producing, our primary focus is on improving care by providing a direct consultation service to our patients.”
Pizzitola and Robinson proposed a pilot phase for the project and designed an Internal Review Board (IRB) survey to collect feedback from patients to measure the clinic’s effectiveness throughout this phase. As the logistics came together, the proposal for the consultation clinic slowly gained administrators’ support.
Finding Space and Time
From there, Robinson and Pizzitola worked with Mayo’s IT department to build an electronic interface in the EMR that would allow clinicians to order the consultations. They also spoke directly with referring physicians to develop the clinic’s workflow, including when and where to consult with patients. Together, they decided that a referrer could order a consultation any time after a woman with dense breast tissue has a normal screening mammogram and that the consultation would occur as a separate visit.
While it made logistical sense to hold the consultations in Mayo’s breast clinic, which also houses oncology, breast surgery, and women’s health providers, it wasn’t feasible to dedicate an exam suite or conference room exclusively to dense breast consultations. Instead, the clinic had to share space with the other specialties in the center.
“We had to get other clinicians in the breast clinic on board with the fact that we’d be using suites just like they do,” Robinson says. “It wasn’t a huge hurdle, but because imaging consultations were such a new concept, we had to sort out the scheduling and patient flow with other providers to make it as efficient as possible for everyone.”
Since the breast imaging department didn’t have the bandwidth to staff the clinic every day, Robinson and Pizzitola began scheduling appointments for a few hours at a time, before dedicating a full day or two per week. This required support from the rest of the radiology staff, who had to cover Pizzitola and Robinson’s time away from reading mammograms.
“Early on, I handled most of the visits, but if I couldn’t get off clinical service, Dr. Pizzitola volunteered some of his administrative time,” Robinson says. “There were a lot of technical kinks to figure out, such as learning how to sign consultation notes and learning how to bill in our EMR, so the pilot allowed us to streamline the workflow before expanding the program.”
Educating Patients
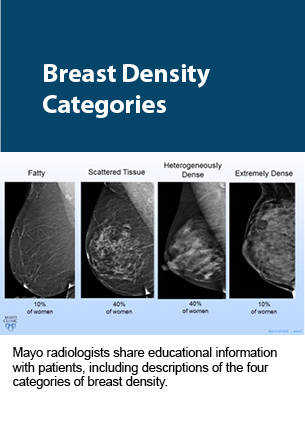
With the guidance and approval of women’s health providers, Robinson developed a slideshow presentation to share with patients during the consultations. “As breast radiologists, we have quite a bit of experience discussing findings as they relate to imaging and recommendations for biopsy. That said, we have little experience with formal clinical consultations,” Pizzitola says. “We collaborated with referring providers to translate our imaging expertise surrounding breast density and available adjunct examinations into an understandable level that could be easily dispensed to patients.”
The presentation explains the four categories of breast density and illustrates how dense tissue and cancer appear in various types of imaging. These visual aids guide the discussion between radiologists and patients about supplemental screening options — such as whole-breast ultrasound, contrast-enhanced MRI, molecular breast imaging (MBI), and contrast-enhanced mammography — while addressing common questions, such as radiation dosage and costs that may not be covered by insurance.
The clinic helps patients compare supplemental screening options and make decisions about their next steps. “It was life-changing for me to see the examples of dense breast tissue in a normal mammogram, and then to see a tumor revealed in an MBI,” says Ochenkoski, who had a post-consultation MBI, which came back normal. “I saw how additional imaging can literally save women’s lives, because a cancerous tumor showing up on an MBI com-pared to a regular mammogram could mean the difference between Stage 2 and Stage 4 disease.”
At the end of the consultation, if the patient decides to pursue a secondary exam, the radiologist can immediately schedule it while charting the visit — copying the referring physicians in the EMR so they receive notifications about the order and the results. Alternatively, if the patient requests more time to consider the next steps, the radiologist simply notes which options they discussed to keep the referring physician apprised.
“It’s important that the referring physicians stay in the loop with our recommendations because they’re the ones tracking each woman’s health,” Robinson says. “Plus, it’s reassuring for the patient to know that we’re all connected so we can take care of them as a team.”
Expanding the Reach
The first patients and referring physicians who used the dense breast consultation clinic gave it positive reviews in surveys and emails. “It filled a gap that we’ve seen since states started mandating these breast density notifications,” Kling says. “It’s a great service that we can refer patients to, because they have concerns and questions that general physicians, can’t always answer. The program allows radiologists to provide those answers directly to patients, who can use that information to decide their next steps.”
Within six weeks after launching the program with five referring physicians, Pizzitola opened it up to the rest of the Mayo Clinic in Arizona. He sent an email to the internal referring provider base, detailing what the new clinic offered and how it could benefit patients and physicians. “I included screenshots showing them where to find the dense breast notification in mammography reports and which buttons to click in the EMR to order a consultation,” he says.
Once the clinic opened to general practitioners beyond women’s health, the appointment schedule filled quickly. As Robinson’s fellowship drew to a close, the clinic needed additional resources to meet the increasing demand. Pizzitola asked the department’s other breast imaging subspecialists to get involved, and they began shadowing Robinson to observe the flow of the conversations and the logistics of charting the consultations in the EMR.
After Robinson moved to Mayo Clinic’s Florida location for a staff breast imaging position, Pizzitola also engaged the new breast imaging fellow who took her place. Now, the fellow and the three dedicated breast imagers rotate clinic hours to offer appointments six or seven days a month. They schedule consultations in one-hour time slots, but most conversations last between 30–45 minutes. On average, the clinic sees six to eight patients per day — totaling about 40–50 each month.
“It has become incredibly popular,” says Pizzitola, noting that in November of 2019 the clinic was already scheduling through February of 2020. “But we’re limited by our radiologists’ bandwidth because reading film is still the priority.”
To help, the department is hiring an additional breast radiologist who will participate in the clinic. After the pilot study concludes, Pizzitola plans to shorten the length of consultation visits by streamlining the presentation and refining the target referral demographics based on the patient’s personal history and other risk factors.
Producing Results
The pilot phase and IRB portion of the program won’t conclude until 200 patients have visited the clinic and sufficient data has been collected. Pizzitola plans to publish the survey results and present the data at The Society of Breast Imaging meeting next spring. As of mid-September of 2019, the clinic had seen 140 patients. Of those, 104 patients completed IRB surveys before and after their visits, revealing significant early results.

“We’ve had really positive feedback, both objectively, looking at the information they learned, and subjectively, asking about the usefulness of these visits,” Robinson says. “Before the consultation, about 60% of patients knew that breast density affects breast cancer risk and detection, and afterward, 92% got those questions correct.”
About 89% of patients said they were very satisfied with the consultation experience, and 92% agreed that they left with the knowledge to make an informed decision about their supplemental screening options. In total, consulting radiologists recommended some type of supplemental screening to 101 patients, and 71 of those exams have been performed so far. These secondary exams have not yet detected any additional cancers.
“The goal was never to get patients to do additional imaging. It’s about doing the right exams on the right subset of patients who really need additional imaging,” Pizzitola says. “The way we quantify return on investment is knowing that we’re improving patient care by filling the gap of knowledge around breast density. This empowers women to take charge of their own care by understanding what options are available and making informed decisions.”
The Dense Breast Consultation Clinic also gives radiologists a more direct role in interacting with patients. “The perception of radiologists as dark room readers is outdated,” Robinson says. “Thanks to Imaging 3.0, we are recognizing that if there is a gap in patient care, radiologists can add value beyond reading exams and doing procedures.”
By taking the time to educate patients, radiologists in the dense breast consultation clinic are promoting the importance of imaging. “I finally have an answer instead of fearing the worst,” Ochenkoski says. “I’d never met a radiologist before, so it’s important to get them out in front of patients so we can see who’s making decisions for our care. I now consider the radiologist part of my care team, and I think that’s a missing link in women’s care.”

