One program relies on patient navigators to reach as many patients as possible for colon cancer screening.
- Despite colorectal cancer being the third-leading cause of cancer death, many eligible patients do not get screened. The incidence and mortality rate of colorectal cancer is even higher in underrepresented minority populations.
- A viable alternative to colonoscopy, computed tomographic colonography (CTC) can provide access to patients, yet many patients and referring physicians don’t know that it’s an available option.
- The CTC program at UT Southwestern Medical Center in Dallas uses a patient navigator, personal reminders, and other tools to increase awareness of the test and ensure that patients do not fall through the cracks.
Listen to a Bulletin podcast episode to hear more from Cecilia Brewington, MD, about CTC.
When Marvel star Chadwick Boseman died of colorectal cancer (CRC) in 2020 at the age of 43, fans were shocked not only be-cause he kept his battle with CRC private but also because he was so young. While Boseman’s untimely passing was a surprise to many, the cause of his death is actually quite common. CRC is the third most-deadly cancer in the U.S. — and it’s on the rise among young adults. One in five cases of CRC are in patients between the ages of 20 and 54.1
These numbers are even greater for minority populations. The incidence of CRC among Black Americans is 20% higher than among White Americans, and the CRC mortality rate is also higher: 40% more deaths occur among Black populations than White populations. But race isn’t the only factor. CRC is also 40% more prevalent among people with a lower socioeconomic status than those of a higher socioeconomic status.2
One reason for these disparities is lower screening rates among these groups, says Cecilia C. Brewington, MD, FACR, professor of radiology and vice chair of operations in the department of radiology at UT Southwestern Medical Center in Dallas (UT Southwestern). “Patients don’t undergo colonoscopy screening for a variety of reasons,” she explains. “A big factor is that it requires anesthesia, which means that patients cannot go to work or drive for the rest of the day. Taking time off work, lining up child care, and finding someone to accompany them to their screening appointment can be a lot to ask of patients, especially those of lower socioeconomic status. Some patients also avoid screening for cultural reasons, or they might be afraid.”
Computed tomographic colonography (CTC) can help ease many of these concerns and make it easier for patients to undergo screening for CRC. While stool tests offer non-invasive colon cancer screening, these tests typically show cancer that already exists; direct visualization tests, such as CTC and colonoscopy, can detect polyps before they progress to cancer.3 Recognizing this, Brewington formally established a CTC program at UT Southwestern in 2018 to reach the hospital’s diverse patient population. “We serve a diverse population of patients with a diverse set of needs,” says Brewington. “If multiple options are available for screening, we should provide them.”
“Ultimately, the trial and other research proved that CTC was worth investing in. As the CT technology continued to improve from 16 slice to higher multi-slice scanners and detectors improved, the resolution improved for both 2D and 3D imaging. Re-search studies over time showed progressively improved CTC sensitivities into the 90th percentile for 1cm or greater sized lesions/polyps, which is equivalent to colonoscopy’s efficacy,” says Brewington. As a result, Brewington’s department offered the screening test for patients but did not provide any patient navigation services around it.
Over the next decade, Brewington noticed that although CTC was a valuable screening option, few patients used it and few referring physicians were aware of it. Brewington saw how effective the mammography screening program was at UT South-western: Patients seemed at ease with the breast imaging radiologists, and many returned for their annual screenings without issue. She started speaking with her breast imaging colleagues about their process, which ultimately changed her views on screening.
“I started to understand I couldn’t just offer the test and expect patients to come,” Brewington says. “There had to be an entire program, including screening reminders, information about screening to help patients understand the procedure and their results, and other ways to streamline the process as much as possible for patients. CTC could be a valuable tool for patients concerned about colonoscopy — one that might increase CRC screening rates — if we could just get patients to use it.”
Brewington decided that the CRC screening program with CTC would follow a similar approach to patient engagement as mammography screening. In addition to exam reminders, she determined that the program would include intake forms to help patients determine if they are at above-average risk of colon cancer and staff who would notify patients of test results.
Brewington worked with several of her colleagues in the department to write scripts for explaining CRC screening to patients and patient-friendly reminders. Initially, radiology department administrative staff and technologists led these patient engagement efforts, but Brewington knew it would be important to add dedicated patient navigators to the program to provide critical information about the procedure to patients and help guide them through the screening process. But she needed both funding and approval from leadership.
To that end, Brewington and a gastroenterology colleague created a business plan that showed the value of CRC screening and hiring a patient navigator. She pointed out that because UT Southwestern is an accountable care organization, it could use CRC screening as a quality metric under the Merit-Based Incentive Payment System. She also noted that the program could count toward the Healthcare Effectiveness Data and Information Set metric, which private insurers use to measure a health center’s performance on important dimensions of care and service, such as effectiveness and accessibility of care.
Brewington and her colleague presented the plan to the chair of the oncology program and to the executive vice president of health system affairs at UT Southwestern. “Our oncology chair was already interested in increasing screening options, so it was an easy sell,” Brewington recalls. “The executive vice president was more skeptical about the return on investment, but having a sound business plan that showed multiple advantages helped convince him.”
Garnering support for a CTC screening program also required outreach to other care partners to ensure that other programs would refer eligible patients for CTC. Brewington and fellow radiologists met with additional gastrointestinal and oncology physicians to help them understand the value of CTC as a screening tool that could be offered in addition to colonoscopy. During small group, divisional, and departmental meetings she spoke about CTC’s specificity and sensitivity rates as well as how it might be able to reach the 30% of eligible patients who do not get screened.
In hiring a patient navigator, Brewington says the most important criteria was their passion. “I wanted someone who really understood the importance of preventing deaths as a result of the program,” she says. Once she hired Law, Brewington invited him to attend the National Colorectal Cancer Roundtable meeting with her to further acquaint him with the screening procedure process and understand the value of CRC screening. “Being there with people who are equally passionate about ending CRC deaths gets you excited about the mission,” notes Brewington. She and Law have continued to attend subsequent national meetings.
Now, when a patient calls to schedule an appointment, Law walks them through the entire screening process. He starts by reviewing an intake form with the patient to ensure that CTC is the right procedure for them. (Patients who are at high risk for CRC or who have other diseases, such as Crohn’s, should undergo a colonoscopy so that any found polyps can be removed immediately, Brewington notes.) He then discusses the procedure and answers the patient’s additional questions.
Law also determines if the patient can pick up the tagging agents, which they must ingest prior to the test. If the patient lives too far away from the medical center to pick up the agents, UT Southwestern will mail them directly to the patient. “We want everything to be as seamless as possible for the patient, from start to finish,” Law says.
After the procedure, Law mails a letter to the patient that outlines their results, no matter the outcome. In cases with serious findings, a radiologist will first contact the provider who ordered the test or the patient’s primary care physician (PCP). “PCPs need to feel secure knowing the patient will be managed appropriately from referrals to follow-up of abnormal findings to re-minders for the next screening event,” Brewington says. She adds that this trust between the referring provider and the radiologist is a key component of a program’s success. “Patients trust their PCPs. If a PCP refers a patient to a CTC screening, they’re more likely to follow up. PCPs also play a role in letting patients know this option even exists.”
In addition to walking patients through their exams, Law uses a spreadsheet to track when patients are due for their CTC screenings, which should occur at a minimum of every five years. When a patient is due for their next screening, he calls, some-times two or three times, to remind them to schedule. If Law is unable to contact a patient, he sends the patient a reminder letter and notifies their PCPs that they are overdue for screening and haven’t made an appointment. Each time he contacts the patient, he notes it in the spreadsheet and patient chart.
Automated screening reminders also appear in the electronic health record so that any UT Southwestern provider who sees a patient who is due for screening can remind them to make an appointment. This tool allows Law to dedicate most of his time to patients who are no-shows or who do not follow up. “It’s not the person who is diligent about coming into the hospital that we’re concerned about,” Brewington says. “We need to focus on those who don’t show or who feel they’re too busy to get screened to increase the overall number of screening candidates.”
Brewington and her colleagues are also working to ensure that the program is accessible in part by offering Saturday appointments and screening at different locations. CTC does not require a radiologist to be on site (only a trained technologist and a CT machine), so like mammography and other types of screening, it can be conducted at off-site locations, which is particularly helpful as the program expands into rural areas of Texas, Brewington notes.
Law also works closely with the other colon cancer screening navigators to educate them about the program so that if they encounter a patient who might benefit from CTC, they’ll know to recommend it to the ordering physician. Law has created a presentation to showcase the program for ordering physicians inside and outside of UT Southwestern. “The biggest thing is letting people know that it’s available,” he says. “A lot of people assume their only options are colonoscopy or the fecal tests.”
Brewington and Law’s work has paid off. Law estimates that the number of CTC screenings has increased about 20% each year since he joined the program in 2018. Although they have not calculated the total return on investment of the program, Brewington believes that any increase in appropriate screenings is a valuable investment. “The best way to take care of a patient population is to keep them healthy — that includes screening for cancers,” she says.
The ACR Colon Cancer committee, of which Brewington is a member, works tirelessly to encourage CMS to take a different stand. Members of the committee also write letters and meet with legislators about CRC screening and have testified about the efficacy of CTC on Capitol Hill.
“CTC presents a huge opportunity to reach those who may not otherwise undergo CRC screening,” Brewington says. “We need to help Congress and the USPSTF understand that Medicare should cover CTC. By giving patients more options, we can eliminate more barriers to access, meaning that more patients may be willing to be screened.”
When Marvel star Chadwick Boseman died of colorectal cancer (CRC) in 2020 at the age of 43, fans were shocked not only be-cause he kept his battle with CRC private but also because he was so young. While Boseman’s untimely passing was a surprise to many, the cause of his death is actually quite common. CRC is the third most-deadly cancer in the U.S. — and it’s on the rise among young adults. One in five cases of CRC are in patients between the ages of 20 and 54.1
These numbers are even greater for minority populations. The incidence of CRC among Black Americans is 20% higher than among White Americans, and the CRC mortality rate is also higher: 40% more deaths occur among Black populations than White populations. But race isn’t the only factor. CRC is also 40% more prevalent among people with a lower socioeconomic status than those of a higher socioeconomic status.2
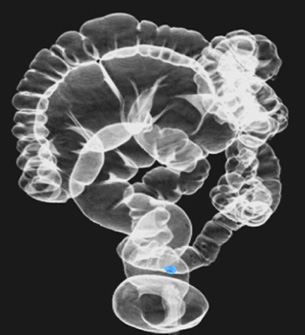 Computed tomographic colonography is an alternative to traditional colonography that doesn’t require anesthesia, making it easier for patients to undergo recommended screening. |
Computed tomographic colonography (CTC) can help ease many of these concerns and make it easier for patients to undergo screening for CRC. While stool tests offer non-invasive colon cancer screening, these tests typically show cancer that already exists; direct visualization tests, such as CTC and colonoscopy, can detect polyps before they progress to cancer.3 Recognizing this, Brewington formally established a CTC program at UT Southwestern in 2018 to reach the hospital’s diverse patient population. “We serve a diverse population of patients with a diverse set of needs,” says Brewington. “If multiple options are available for screening, we should provide them.”
Implementing CTC
Before establishing a formal program, UT Southwestern began offering diagnostic CTC in 2004 due to a research interest in the emerging technology. Several of Brewington’s gastroenterology colleagues approached her about learning to read CTCs as part of a multi-institutional trial to determine whether CTC was viable as a screening option. The gastroenterologists agreed with Brewington that, if successful, CTC could be used as a complementary program. Radiologic technologists were also trained to perform the exam properly.“Ultimately, the trial and other research proved that CTC was worth investing in. As the CT technology continued to improve from 16 slice to higher multi-slice scanners and detectors improved, the resolution improved for both 2D and 3D imaging. Re-search studies over time showed progressively improved CTC sensitivities into the 90th percentile for 1cm or greater sized lesions/polyps, which is equivalent to colonoscopy’s efficacy,” says Brewington. As a result, Brewington’s department offered the screening test for patients but did not provide any patient navigation services around it.
 Cecilia C. Brewington, MD, FACR, professor of radiology and vice chair of operations in the department of radiology at UT Southwestern Medical Center in Dallas, led development of the CTC program. |
“I started to understand I couldn’t just offer the test and expect patients to come,” Brewington says. “There had to be an entire program, including screening reminders, information about screening to help patients understand the procedure and their results, and other ways to streamline the process as much as possible for patients. CTC could be a valuable tool for patients concerned about colonoscopy — one that might increase CRC screening rates — if we could just get patients to use it.”
Starting the Program
To start a full-fledged screening program, Brewington approached her colleague Phil Evans, MD, FACR, chair of the breast imaging division, to learn about the various ways the mammography program helps encourage patients to come in for their annual screenings, from exam reminders to patient navigators who walk patients through the entire screening process.Brewington decided that the CRC screening program with CTC would follow a similar approach to patient engagement as mammography screening. In addition to exam reminders, she determined that the program would include intake forms to help patients determine if they are at above-average risk of colon cancer and staff who would notify patients of test results.
Brewington worked with several of her colleagues in the department to write scripts for explaining CRC screening to patients and patient-friendly reminders. Initially, radiology department administrative staff and technologists led these patient engagement efforts, but Brewington knew it would be important to add dedicated patient navigators to the program to provide critical information about the procedure to patients and help guide them through the screening process. But she needed both funding and approval from leadership.
To that end, Brewington and a gastroenterology colleague created a business plan that showed the value of CRC screening and hiring a patient navigator. She pointed out that because UT Southwestern is an accountable care organization, it could use CRC screening as a quality metric under the Merit-Based Incentive Payment System. She also noted that the program could count toward the Healthcare Effectiveness Data and Information Set metric, which private insurers use to measure a health center’s performance on important dimensions of care and service, such as effectiveness and accessibility of care.
Brewington and her colleague presented the plan to the chair of the oncology program and to the executive vice president of health system affairs at UT Southwestern. “Our oncology chair was already interested in increasing screening options, so it was an easy sell,” Brewington recalls. “The executive vice president was more skeptical about the return on investment, but having a sound business plan that showed multiple advantages helped convince him.”
Garnering support for a CTC screening program also required outreach to other care partners to ensure that other programs would refer eligible patients for CTC. Brewington and fellow radiologists met with additional gastrointestinal and oncology physicians to help them understand the value of CTC as a screening tool that could be offered in addition to colonoscopy. During small group, divisional, and departmental meetings she spoke about CTC’s specificity and sensitivity rates as well as how it might be able to reach the 30% of eligible patients who do not get screened.
Adding a Navigator
With leadership and other care partners on board and funding approved, Brewington hired a patient navigator for the program. Thomas Law, who previously worked for UT Southwestern as a registered nurse, is the first CTC patient navigator, although he will soon be training another navigator to join the ranks. Thomas Law, CTC patient navigator, walks patients through the entire CTC process to make the screening as seamless for them as possible. |
Now, when a patient calls to schedule an appointment, Law walks them through the entire screening process. He starts by reviewing an intake form with the patient to ensure that CTC is the right procedure for them. (Patients who are at high risk for CRC or who have other diseases, such as Crohn’s, should undergo a colonoscopy so that any found polyps can be removed immediately, Brewington notes.) He then discusses the procedure and answers the patient’s additional questions.
Law also determines if the patient can pick up the tagging agents, which they must ingest prior to the test. If the patient lives too far away from the medical center to pick up the agents, UT Southwestern will mail them directly to the patient. “We want everything to be as seamless as possible for the patient, from start to finish,” Law says.
Tracking Patients
Once Law schedules a procedure, he mails the patient a letter explaining where the CTC will take place, along with directions to the location. He also includes his direct phone number should the patient have additional questions. “It’s a lot of information for a patient to absorb at once,” Law says. “I send over a copy of everything we discussed on the call and make sure they know they’re welcome to reach out.”After the procedure, Law mails a letter to the patient that outlines their results, no matter the outcome. In cases with serious findings, a radiologist will first contact the provider who ordered the test or the patient’s primary care physician (PCP). “PCPs need to feel secure knowing the patient will be managed appropriately from referrals to follow-up of abnormal findings to re-minders for the next screening event,” Brewington says. She adds that this trust between the referring provider and the radiologist is a key component of a program’s success. “Patients trust their PCPs. If a PCP refers a patient to a CTC screening, they’re more likely to follow up. PCPs also play a role in letting patients know this option even exists.”
In addition to walking patients through their exams, Law uses a spreadsheet to track when patients are due for their CTC screenings, which should occur at a minimum of every five years. When a patient is due for their next screening, he calls, some-times two or three times, to remind them to schedule. If Law is unable to contact a patient, he sends the patient a reminder letter and notifies their PCPs that they are overdue for screening and haven’t made an appointment. Each time he contacts the patient, he notes it in the spreadsheet and patient chart.
Automated screening reminders also appear in the electronic health record so that any UT Southwestern provider who sees a patient who is due for screening can remind them to make an appointment. This tool allows Law to dedicate most of his time to patients who are no-shows or who do not follow up. “It’s not the person who is diligent about coming into the hospital that we’re concerned about,” Brewington says. “We need to focus on those who don’t show or who feel they’re too busy to get screened to increase the overall number of screening candidates.”
Engaging New Patients
As part of that focus, Law manages outreach to educate as many patients as possible about the program and the benefits of regular colorectal cancer screening. Radiologists at UT Southwestern use various avenues to reach all patient populations. “We’ve done some television broadcasts, and we send public service announcements out over different radio stations — from R&B to country and western,” Brewington says.Brewington and her colleagues are also working to ensure that the program is accessible in part by offering Saturday appointments and screening at different locations. CTC does not require a radiologist to be on site (only a trained technologist and a CT machine), so like mammography and other types of screening, it can be conducted at off-site locations, which is particularly helpful as the program expands into rural areas of Texas, Brewington notes.
Law also works closely with the other colon cancer screening navigators to educate them about the program so that if they encounter a patient who might benefit from CTC, they’ll know to recommend it to the ordering physician. Law has created a presentation to showcase the program for ordering physicians inside and outside of UT Southwestern. “The biggest thing is letting people know that it’s available,” he says. “A lot of people assume their only options are colonoscopy or the fecal tests.”
Brewington and Law’s work has paid off. Law estimates that the number of CTC screenings has increased about 20% each year since he joined the program in 2018. Although they have not calculated the total return on investment of the program, Brewington believes that any increase in appropriate screenings is a valuable investment. “The best way to take care of a patient population is to keep them healthy — that includes screening for cancers,” she says.
Advocating for Medicare Coverage
Despite its high sensitivity and easy access, CTC is not affordable for all patients. Many private insurers cover the cost of screening for adults aged 45-75 under the Affordable Care Act’s requirement that insurance cover screenings with A or B ratings from the United States Preventive Services Task Force (USPSTF).4 However, despite USPSTF’s guidance that CTC should be widely available to all eligible candidates, as of April of 2022, the Centers for Medicare & Medicaid Services (CMS) does not reimburse for screening CTC unless Medicare patients meet specific criteria. Patients who do not meet the criteria must pay out of pocket for the test.The ACR Colon Cancer committee, of which Brewington is a member, works tirelessly to encourage CMS to take a different stand. Members of the committee also write letters and meet with legislators about CRC screening and have testified about the efficacy of CTC on Capitol Hill.
“CTC presents a huge opportunity to reach those who may not otherwise undergo CRC screening,” Brewington says. “We need to help Congress and the USPSTF understand that Medicare should cover CTC. By giving patients more options, we can eliminate more barriers to access, meaning that more patients may be willing to be screened.”
Endnotes
1. Siegel RL et al. “Colorectal Cancer Statistics, 2020.” CA: A Cancer Journal for Clinicians. 2020; 70(3):145-164. Available at: https://acsjournals.onlinelibrary.wiley.com/doi/full/10.3322/caac.21601
2. Brewington CC. “Changing the Storyline.” ACR Bulletin. October 2021. https://www.acr.org/Practice-Management-Quality-Informatics/ACR-Bulletin/Articles/October-2021/Changing-the-Storyline Accessed March 1, 2022.
3. American Cancer Society. “Colorectal Cancer Facts & Figures 2020-2022.” Atlanta: American Cancer Society; 2020. Accessed March 3, 2022. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/colorectal-cancer-facts-and-figures/colorectal-cancer-facts-and-figures-2020-2022.pdf.
4. U.S. Preventive Services Task Force. Final recommendation statement: colorectal cancer: screening. May 18, 2021. Accessed March 3, 2022. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/colorectal-cancer-screening.
Creative Commons
Expanding Colon Cancer Screening by American College of Radiology is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. Based on a work at www.acr.org/imaging 3. Permissions beyond the scope of this license may be available at www.acr.org/Legal.
Share Your Story
Have a case study idea you’d like to share with the radiology community? To submit your idea please click here.
Now It's Your Turn
Follow these steps to begin improving CTC access at your institution, and tell us how you did at imaging3@acr.org or on Twitter with the hashtag #Imaging3:
- Learn how to read CTC through a course like this one that the ACR offers: https://www.acr.org/Lifelong-Learning-and-CME/Education-Center/ct-colonography
- Consider how other programs, like mammography, have successfully engaged patients to increase adherence to screening guidelines. Apply methods that would be especially effective for your patient community.
- Hire a patient navigator to ensure that patient engagement remains a top priority to reduce cancer deaths.
Author
Meghan Edwards, freelance writer
Join the Discussion

Want to join the discussion about how radiologists
can lead quality improvement projects for improved
image ordering? Let us know your thoughts on
Twitter at #imaging3.
#Imaging3 on Twitter
Call for Case Studies
