By Ufara Zuwasti, MD, MSc
PGY-3, Newark Beth Israel Medical Center, Newark, NJ
Advancing Radiology Services in Indonesia: Developing a Global Health Radiology Project
In 2019, just before beginning my PGY-1 training, I started the RAD-AID Indonesia program at the University of Indonesia Faculty of Medicine — Cipto Mangunkusumo Hospital, the institution at which I first began my medical training almost a decade earlier (see Figure 1).

Figure 1. University of Indonesia Faculty of Medicine; Source: https://fk.ui.ac.id/
With nearly 270 million people, Indonesia is the fourth most populous country in the world after China, India and the United States, and the short supply of 1,500 radiologists throughout the country are not equally distributed. Below is my experience developing a global health radiology project in Indonesia.
RAD-AID is a U.S.-based, nonprofit, nongovernmental organization that improves and optimizes access to radiology and medical imaging globally in low-resource settings. A cornerstone of this organization is its Radiology-Readiness Assessment, a systematic data collection tool that thoroughly evaluates radiology infrastructure, staffing and availability of downstream care prior to deciding on an intervention (see Figure 2). This assessment helps RAD-AID and its partners prioritize institutional needs as well as implement and evaluate radiology programs that are sustainable, measurable and scalable.
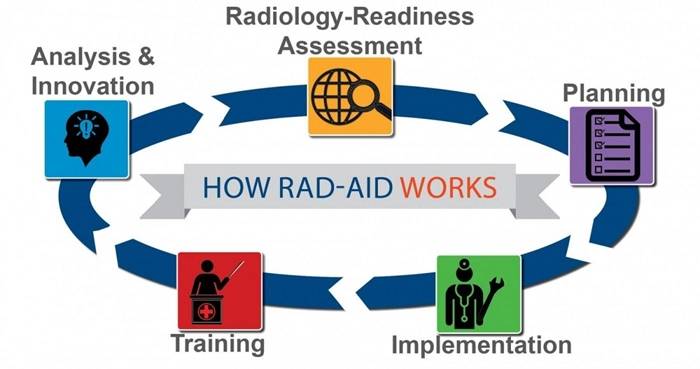
Figure 2. Radiology-Readiness Assessment: A Framework for Implementing Radiology Projects.
One of the most crucial steps to developing a global health radiology project is to choose local champions at the partnering institution who will lead the project in-country, ensuring sustainability. Without a strong local team, it is challenging to manage a project from overseas.
The Radiology-Readiness Assessment collects comprehensive information on all facets of radiology services and examines the healthcare context for the radiology services required to understand how those services are delivered in certain settings. Radiology readiness ensures that any chosen program of assistance will yield the most effect.
With help from Indonesian colleagues, we began the assessment in 2018 and finished in 2019. Our readiness assessment of Cipto Mangunkusumo, a government-run tertiary care hospital, found the following:
- The hospital had over 950 inpatient beds, the occupancy rate of which is greater than 90%.
- The hospital sees about 3,200 outpatients every day.
- The hospital had 19 radiologists, 57 residents, 37 radiologic technologists and 10 radiologic nurses.
- The hospital had no sonographer as sonography services were performed by radiologists and residents.
- All radiology equipment, except for nuclear radiology, were provided through public-private partnership with nongovernmental third parties that oversaw providing, maintaining and repairing the equipment.
- PACS were first installed in 2013.
The radiology department offered all subspecialty services with MSK and abdominal imaging, which were considered to be the leading subspecialties. Interventional radiology was not the institution’s focus due to lack of manpower, equipment and consumables. Furthermore, many procedures weren’t covered by the national health insurance program.
The institution wanted to advance its breast imaging services, although the country did not have a national breast cancer screening program. No well-established fellowship program existed as the current national fellowship program was not hospital-based. The program was supervised by the Indonesian Board of Radiologists, and the requirements for each subspecialty differed from one another. At the time of this article’s publication, the institution had just started its institution-based abdominal fellowship program.
After completion of the readiness assessment, I conducted an analysis with RAD-AID colleagues and Indonesian partners to help prioritize areas of intervention, which in this case were education, healthcare IT and clinical service optimization. We then formulated goals, objectives, action plans, timelines and evaluation metrics into a project document.
In June 2020, we had planned an on-site visit with a multidisciplinary team consisting of a radiology attending, technologist, nurse, resident and U.S. medical student. The trip was canceled, however, due to the COVID-19 pandemic. To maintain our momentum, we decided to kick off the project with Zoom lectures in interventional radiology (IR) and breast imaging topics, as requested by the partnering institution.
For the first IR and breast imaging lecture series, we partnered with the RAD-AID IR team from Weill Cornell Medicine, Thomas Jefferson University Hospital and Lakewood Regional Medical Center in Southern California as well as the RAD-AID Duke Chapter for six months (see Figure 3).

Figure 3. Residents and attendings.
We have plans for on-site, hands-on training for IR and breast imaging services, including an exchange program for residents and attendings, as well as capacity building for quality improvement, scaling diagnostic services and optimizing existing mobile mammography.
The second lecture series will cover body and pediatric imaging, led by the RAD-AID Emory Chapter, as well as topics in breast imaging provided by the RAD-AID Duke Chapter. Our program also features invited lecturers from other institutions, such as Children’s Hospital Los Angeles, Newark Beth Israel Medical Center, University of California San Francisco and Memorial Sloan Kettering Cancer Center.
Recently, the RAD-AID breast imaging program purchased the ACR BI-RADS® Atlas for distribution to all its intervention sites, including Indonesia (See Figures 4 and 5).

Figure 4: Installation of BI-RAD Atlas.

Figure 5: Installation of BI-RAD Atlas.
We also just completed a RAD-AID Readiness Assessment specifically made for breast imaging programs to further analyze current capacity and challenges toward advancing breast imaging services. Discussions are ongoing to provide technical assistance in starting or improving Indonesia’s fellowship programs in breast and body imaging in the future.
An obvious question is, “Given RAD-AID’s mission, why partner with a tertiary care facility instead of a low-resource hospital?” Only a handful of institutions in Indonesia offer radiology residency, and the University of Indonesia Faculty of Medicine (see Figure 1) — Cipto Mangunkusumo Hospital (located in the capital of Jakarta) — supplies most of the country’s radiologists. Furthermore, even though the site is not low resource in terms of radiology modalities, gaps exist in other areas identified in the readiness assessment.
The goal is to create a benchmark for quality education and radiology services in Indonesia. The readiness assessment is not a one-time affair, but rather an ongoing learning process (see Figure 2). Recurring assessments will be conducted following predefined program milestones to further guide whether the chosen interventions are meeting established objectives, as well as to identify new priorities.
Learn more about starting a global health radiology project and radiology readiness. You can also email me at uzuwasti@rad-aid.org.