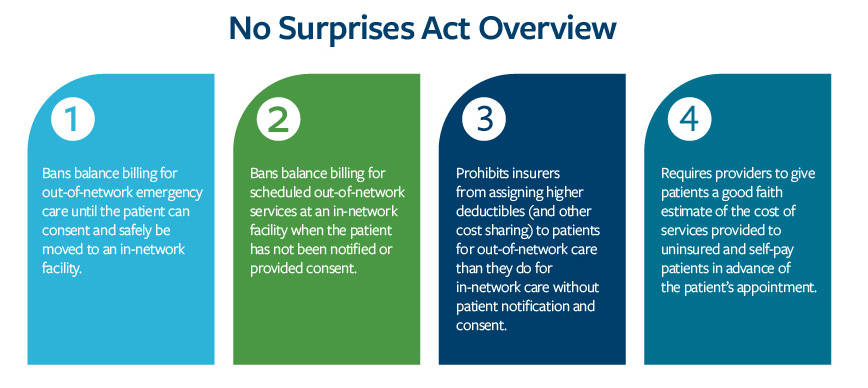
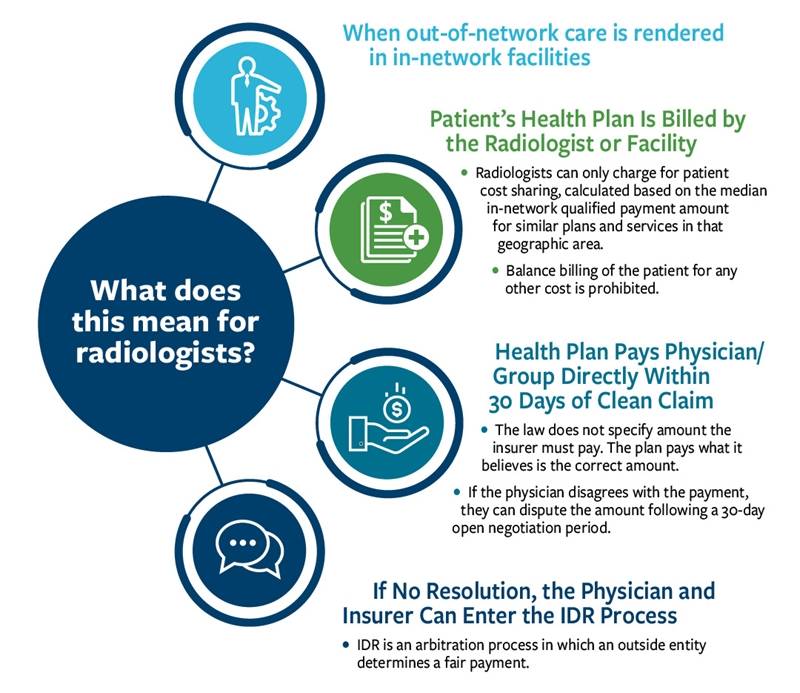
As passed by Congress, the No Surprises Act held patients harmless and created an equitable provider-insurer independent dispute resolution (IDR) process.
The surprise billing interim final rules that took effect Jan. 1, however, ignored the law’s intent that a qualified payment amount (QPA) be among equally weighted factors considered in these disputes.
The rules made the QPA the primary factor over others, creating a benchmark payment that is set by insurers. This will result in narrower provider networks, drastic imaging reimbursement cuts regardless of network status and reduced patient access to care.
Lawsuit News
The American College of Radiology® (ACR®), American College of Emergency Physicians and American Society of Anesthesiologists are suing agencies of the federal government to block parts of the rule implementing the No Surprises Act leaving the patient protections intact.